Retina

Retina Care
At Lexington Eye Associates, we emphasize excellence in eye care.
The retina is the light-sensitive tissue lining the back of our eye. Light rays are focused onto the retina through our cornea, pupil, and lens. The retina converts the light rays into impulses that travel through the optic nerve to our brain, where they are interpreted as the images we see.
Diseases of the Retina
Macular Degeneration
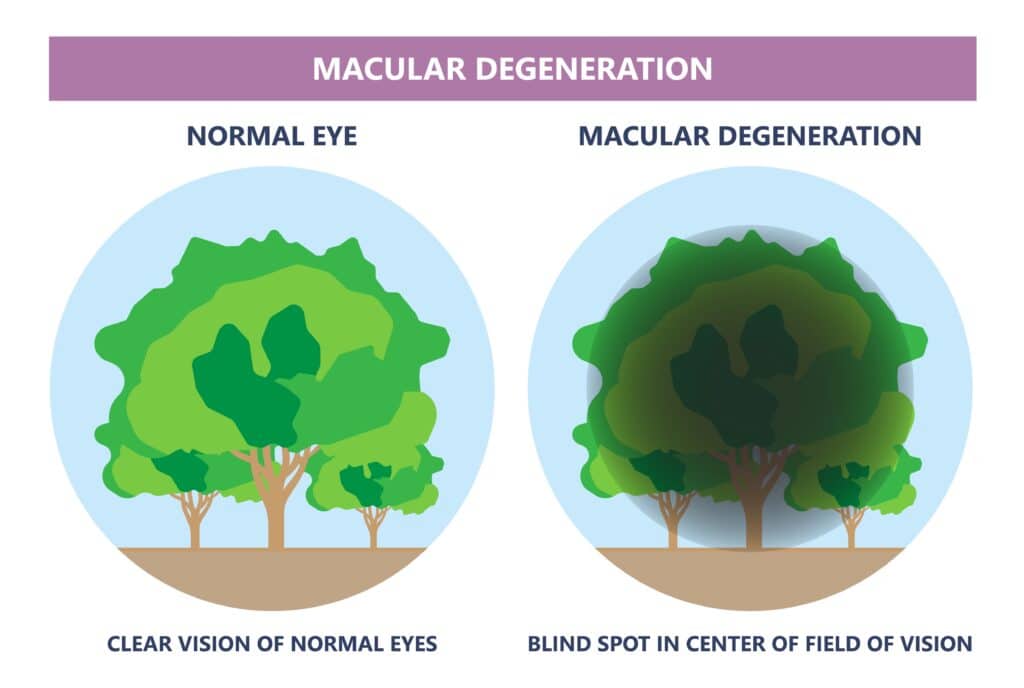
Age-related macular degeneration (ARMD) is a progressive disease of the retina that causes blurring of your central vision. The blurring happens because of damage to the macula, a small area at the back of the eye. The macula helps you see the fine detail in things that your eyes are focusing on. Macular degeneration makes it harder to do things that require sharp central vision, like reading, driving, and recognizing faces. It does not affect side vision, so it does not lead to complete blindness.
The disease is thought to be caused by a combination of genetic and environmental factors, and it is most common in people who are aged 60 and over. ARMD is the leading cause of visual impairment in senior citizens. An estimated 15 million people in the United States have it, and approximately two million new cases are diagnosed annually.
There are two types of macular degeneration: wet and dry. The dry form is, by far, the most common type. The wet form is much less common, but it happens more quickly and is more severe.
Dry ARMD accounts for about nine out of 10 cases of macular degeneration. It develops slowly and causes central vision to become dimmer or blurrier over time. It usually does not cause severe vision loss unless it turns into the wet form.
Wet ARMD accounts for only about one out of 10 cases of macular degeneration. It can cause serious vision loss within months or even weeks. People who have the wet form have the dry form first.
You may have either type in just one eye, but over time, you may get it in the other eye too.
If you have the wet form of macular degeneration, you may have one or more of the following treatments:
These treatments can’t restore central vision, but they may slow down vision loss. If your doctor recommends photodynamic therapy, injections, or laser surgery, it is important to have it done right away.
No one has found a treatment or cure for the dry form of age-related macular degeneration. Antioxidants may protect against age-related macular degeneration by preventing free radicals or unstable oxygen from damaging the retina. Your Lexington Eye ophthalmologist will direct you in the appropriate course of treatment for your specific needs.
Flashes and Floaters
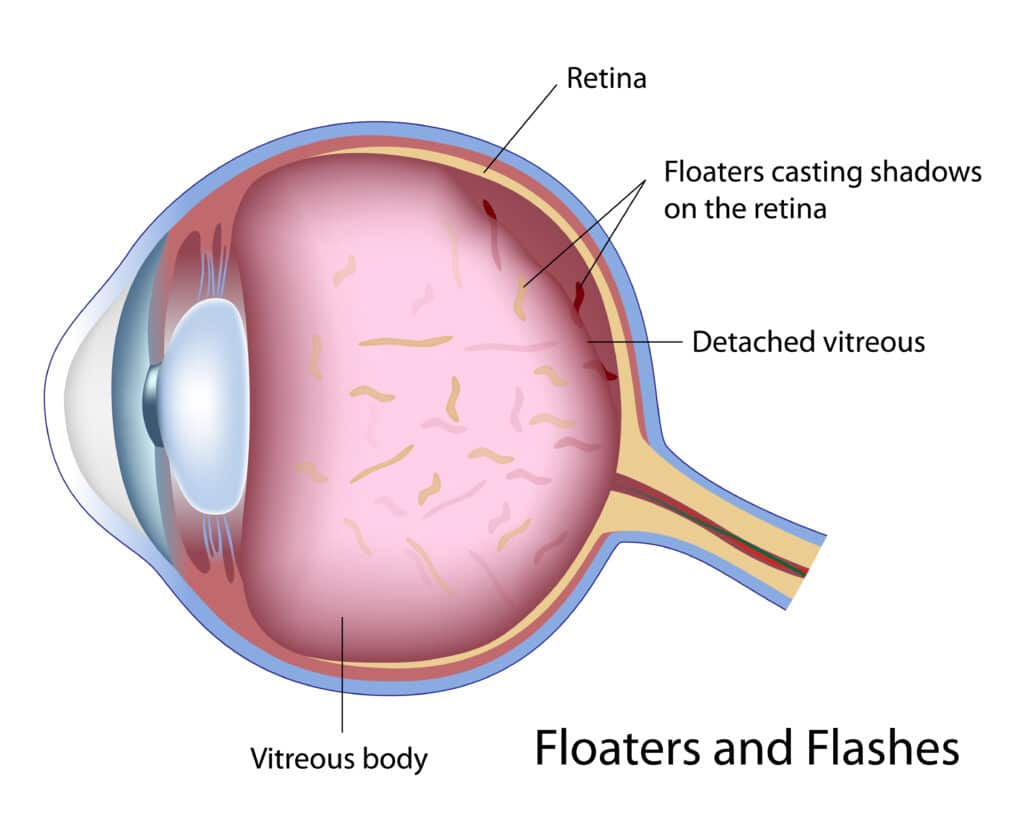
Many people that develop flashes and floaters can get very concerned, and this is normal. Typically, floaters may appear as small specks or dark shadows. These specks can actually move or float around in the visual field. This condition develops from changes in the back of the eye also known as the vitreous cavity.
Symptoms
In most cases, flashes and floaters are caused by age-related changes in the back of the eyes and further changes in the vitreous fluid (gel material). The vitreous fluid gradually becomes more viscous or watery over time. What happens after the age of 30 or so is that the vitreous might be watery enough to swallow clumps of material. This is how the floaters may develop. These clumps of material floating inside the eye can cast shadows on the retina and is why people see floating spots.
Diagnosing Flashes and Floaters
At Lexington Eye Associates, a comprehensive eye examination is conducted to determine if this is a serious issue or a relatively harmless condition. We will use very specialized diagnostic equipment to exam a person’s eyes and look for potential issues related to the retina.
Floaters can be a serious problem. However, in most cases, the problems are not serious. Please consult a retinal specialist at Lexington Eye Associates before trying to diagnose the severity of this condition.
Retinal Tears and Detachments
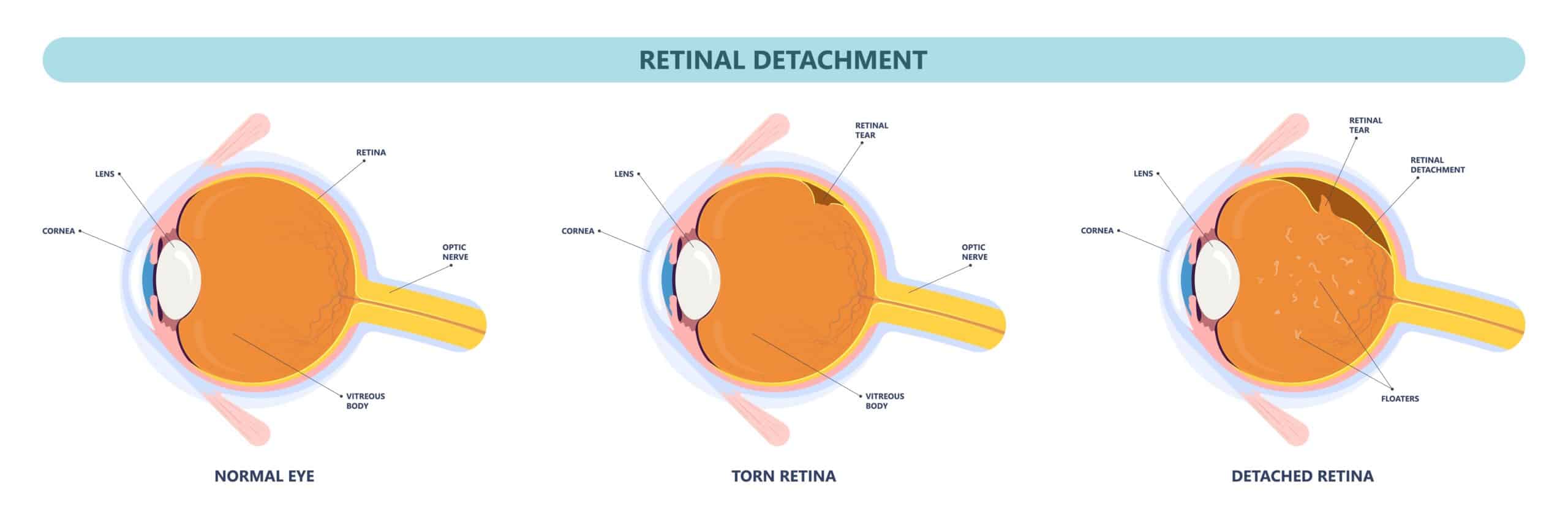
Retinal detachment is a disorder of the eye in which the retina separates from its underlying layer of support tissue. Initial detachment may be localized, but without rapid treatment, the entire retina may detach, leading to vision loss and blindness.
Retinal detachment is a medical emergency.
The retina is a thin layer of light-sensitive tissue on the back wall of the eye. The optical system of the eye focuses light on the retina much like light is focused on the film in a camera. The retina translates that focused image into neural impulses and sends them to the brain via the optic nerve. Occasionally, posterior vitreous detachment, injury or trauma to the eye or head may cause a small tear in the retina. The tear allows vitreous fluid to seep through it under the retina and peel it away like a bubble in wallpaper.
Symptoms of Retinal Detachment
A retinal detachment is commonly preceded by a posterior vitreous detachment which gives rise to these symptoms:
Although most posterior vitreous detachments do not progress to retinal detachments, those that do produce the following symptoms:
Treatment
There are several methods of treating a detached retina, which all depend on finding and closing the breaks which have formed in the retina.






